Guidelines
When to use local vs systemic therapy
Patients with mild, symptomatic cGVHD limited to a single site may often be managed with local therapies alone, such as topical corticosteroids for skin disease. In contrast, systemic immunosuppressive therapy should be considered when cGVHD involves 3 or more organs or when any single organ has a severity score ≥2. Clinical judgment remains essential, and decisions should be individualized based on high-risk features (eg, thrombocytopenia), the underlying transplant indication (malignant vs nonmalignant disease), and the patient’s overall clinical status.1
Early initiation of effective systemic therapy in patients with clinically significant disease may help prevent progression to severe cGVHD and reduce transplant-related mortality (TRM). However, the presence of active or comorbid infections may influence both the timing and intensity of systemic treatment. For patients already receiving immunosuppressive therapy, management may include dose escalation of current agents or the addition of new systemic therapies to improve disease control.1
Because patients with cGVHD—especially those on systemic immunosuppression—are highly immunocompromised, comprehensive infection-prevention measures are a critical component of care.1
First-line systemic therapy for cGVHD
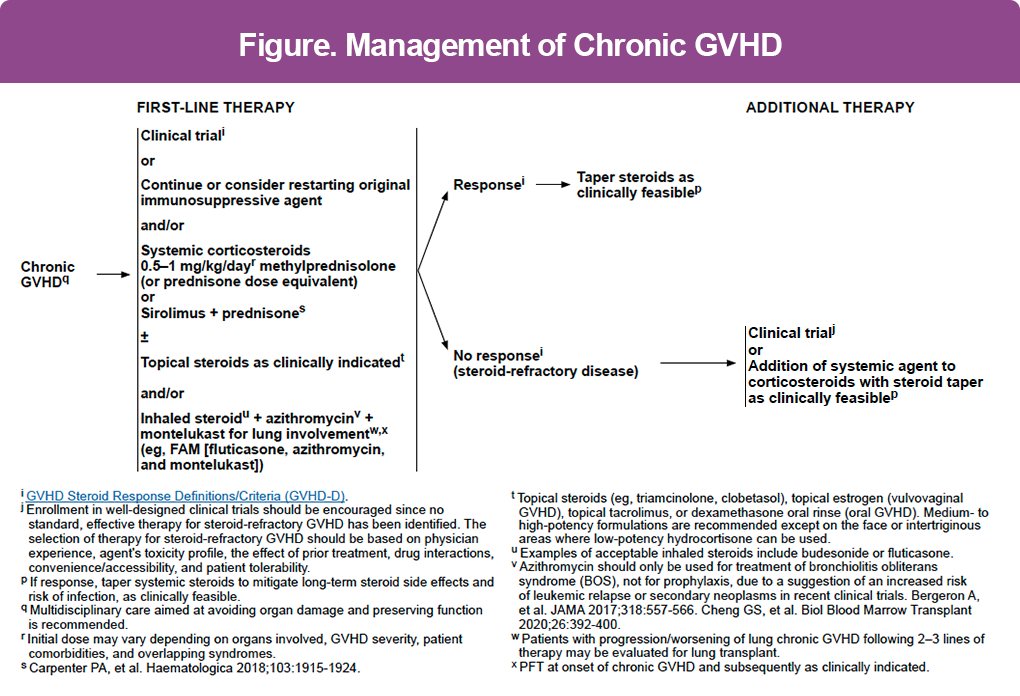
Whenever feasible, enrollment in a well-designed clinical trial is strongly encouraged at all stages of treatment. Standard first-line options include (Figure):
- Continuation, reinitiation, or escalation of the original immunosuppressive agent
- Systemic corticosteroids (prednisone or methylprednisolone 0.5–1 mg/kg/day)
- Sirolimus plus prednisone as an alternative to steroids alone in select patients
Initial steroid dosing should be individualized based on the organs involved, disease severity, and patient comorbidities.2
Organ-directed supportive therapies
Local and inhaled therapies are frequently used alongside systemic treatment2:
- Topical corticosteroids and topical estrogen for vulvovaginal involvement
- Topical tacrolimus or dexamethasone oral rinses for oral cGVHD
- Inhaled steroids or fluticasone, azithromycin, and montelukast (FAM) therapy for lung involvement
- Azithromycin should be reserved for treatment of bronchiolitis obliterans (BOS) only, not for prophylaxis, due to concerns about relapse and secondary malignancies
Assessing response and steroid tapering
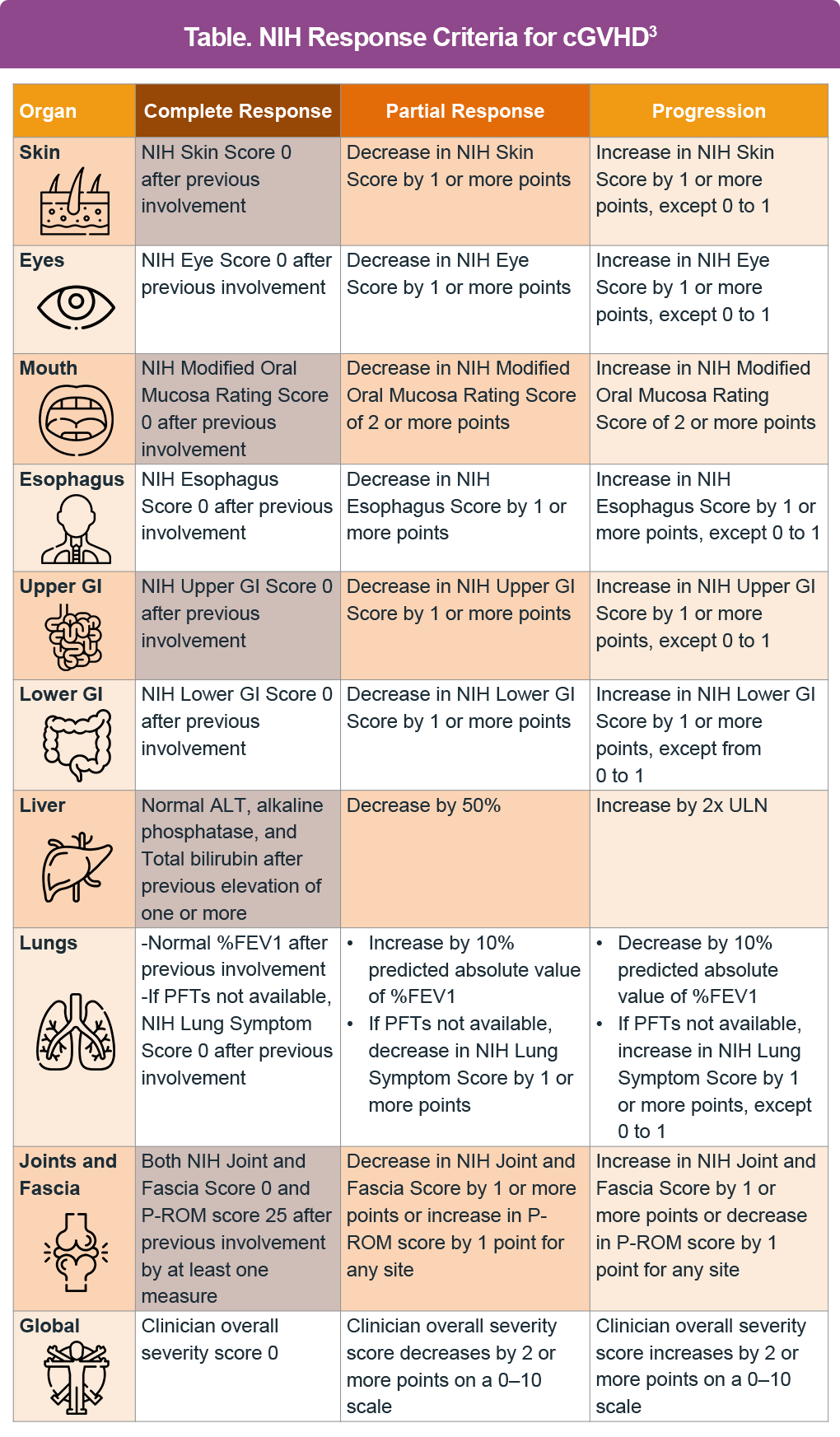
Treatment response should be assessed using the NIH response criteria (Table). In patients who respond, systemic corticosteroids should be tapered slowly and cautiously, as clinically feasible, to minimize long-term toxicity. Patients who successfully respond may still require prolonged maintenance therapy and close monitoring.2
References
Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health Consensus Development Project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and Staging Working Group Report. Biol Blood Marrow Transplant. 2005;11(12): 945-956. https://doi.org/10.1016/j.bbmt.2005.09.004
National Comprehensive Cancer Network (NCCN). Hematopoietic cell transplantation. Version 2.2025. https://www.nccn.org/professionals/physician_gls/pdf/hct.pdf. Accessed 12/13/2025.
Lee SJ, Wolff D, Kitko C, et al. Measuring therapeutic response in chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2015;21(6):984-999. https://doi.org/10.1016/j.bbmt.2015.02.025