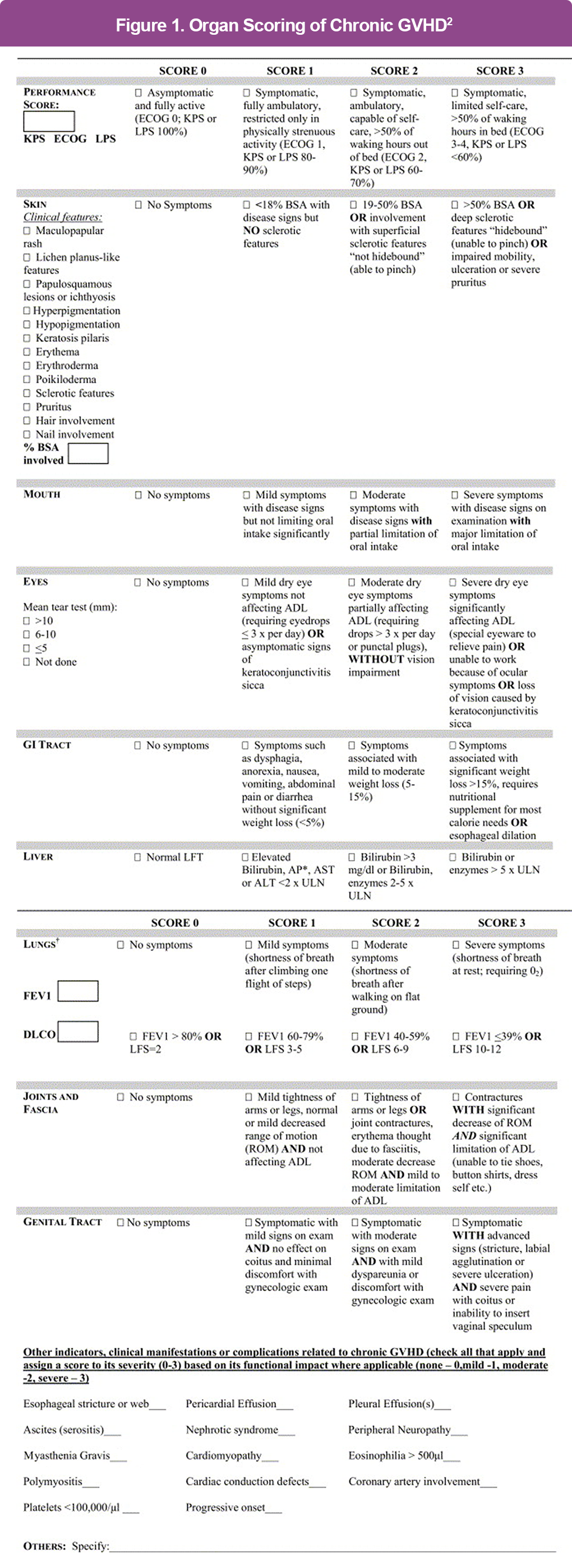
Skin and appendages
(eg, sclerotic changes, lichen-like features, poikiloderma)

Mouth
(eg, lichen-type changes, mucosal atrophy, ulcers)

Female genital tract
(eg, scarring, stenosis, erosions

Gastrointestinal tract and esophagus
(eg, strictures, pancreatic insufficiency)

Liver
(elevated bilirubin or liver enzymes)

Lungs
(bronchiolitis obliterans confirmed by biopsy, imaging, or pulmonary function tests)

Joints, fascia, and muscles
(fasciitis, contractures, myositis)